
Australian researchers Ben Searle and Deborah Starkey from Queensland University of Technology are both exploring better ways to create 3D printed medical models. Their findings were outlined in a recently published “An investigation into the effect of changing the computed tomography slice reconstruction interval on the spatial replication accuracy of three-dimensional printed anatomical models constructed by fused deposition modeling.”
As the important position of 3D printing in the medical field continues to expand, doctors are increasingly relying on 3D printed models and various equipment that can help diagnose, treat, educate, and plan the surgery. In fact, 3D printed models also play a role in the operating room, providing guidance to surgeons who may be performing new or extremely rare procedures. In the past, access to corpses, which was usually the main form of training, was often restricted, and 3D printed models could be made on-demand (and easily modified).
It can greatly reduce the time in the operating room, sometimes up to 20%. Searle and Starkey report; however, “incorrect anatomical manifestations” remain a major problem and major flaw, especially when the results may lead to “unsatisfactory treatment plans.” It has been reported to be flawed, including an understanding of details such as arteries, sub-perforation occlusions, and blurred sutures.
Although CT scans are used for imaging, FDM 3D printing is usually used for 3D printing models due to accessibility and reasonable price:
“FDM printers can be operated and maintained without advanced training and can easily fit into existing workspaces,” explain the authors.
However, in this study, researchers focused on the accuracy and impact of slice width and what improvements can be made:
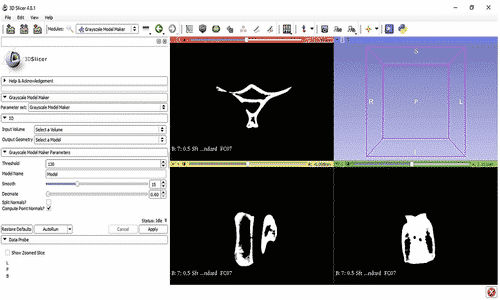
“Slice width has a direct impact on 3D models created from an imaging data set, as higher slice widths result in lower image resolution and anatomical detail. The data from consecutive detector elements in a CT scanner can be combined to reconstruct a number of image series at a range of slice widths from the same raw scan data,” the authors write. “Due to the novel nature of the technology, there is a lack of published literature addressing the influence of reconstruction in CT scan data on the accurate reproduction of 3D‐printed anatomical models, particularly the SRI.”
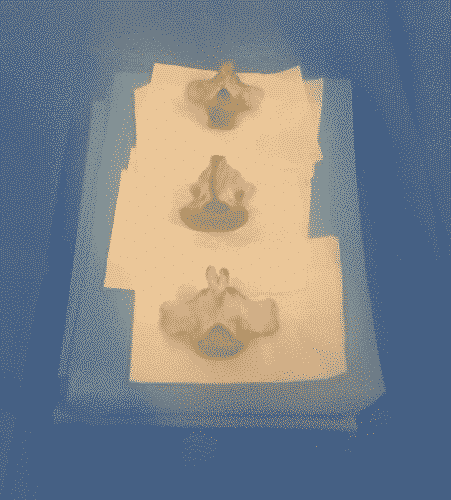
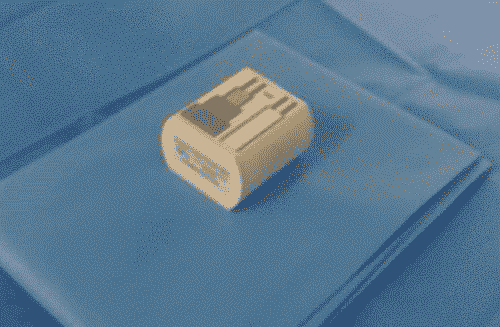
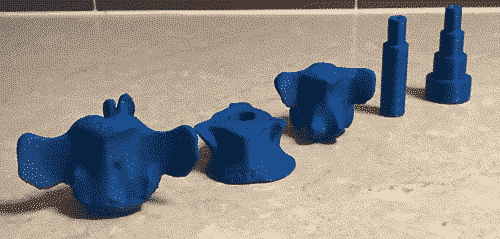
For their study, the authors used three bovine vertebrae (no animals were injured) and an imaging phantom to divide the data into 0.1, 0.3, 0.5, and 1 mm slice reconstruction intervals (SRI).
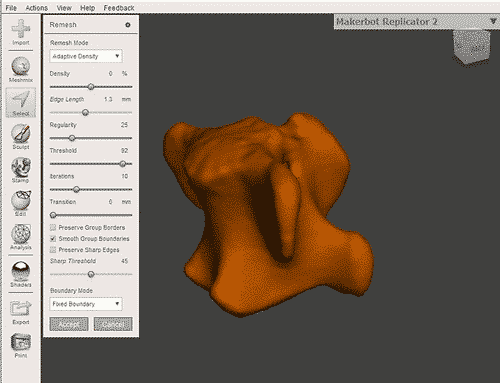
After creating the mesh file to be imported into Meshmixer, the author exported the file to Malyan M200 (XY resolution 0.011 mm, layer resolution 0.1 mm and nozzle width 0.4 mm), and used it in the 3D printing process support.
The manufactured samples are considered “highly realistic” and “suitable for measurement and analysis”. However, the researchers also pointed out that during the slicing process, when the SRI used by the model is less than the main limiting factor for acquiring the spatial resolution of the slicing or printer, the accuracy of the model will decrease. For the following reasons, the use of larger SRI will also lead to reduced accuracy:
- Sum of volume average effects
- Print error
- Handling errors
- Loss of spatial resolution
The authors also point out that even the most accurate 3D models they produce have “an average deviation of about 0.5 mm.”
“However, the spatial resolution error of FDM printers can be significant relative to the acquisition slice width and SRI distances due to printer nozzle width limitations. This is particularly applicable in this study where the FDM printer nozzle width of 0.4 mm is similar to the acquisition slice width of 0.5 mm,” explained the authors.
“This study has successfully achieved research aims by demonstrating that changing the SRI influences the spatial replication accuracy of 3D‐printed anatomical models. It has also demonstrated that a benefit exists in using a SRI equal to or less than the primary limiting factor of either the acquisition slice width or printer capabilities by optimizing the replication accuracy of the model whilst minimizing the digital size of the data and required processing time investment. Consequently, this study can help refine 3D printing protocols in medical and tissue engineering applications and help practitioners to create accurate reproductions of anatomy for various teaching and clinical purposes.”
As 3D printed models continue to bring particular benefits to medical professionals, they are used to assist hip surgery, pediatric orthopedic surgery, and to study congenital heart disease.